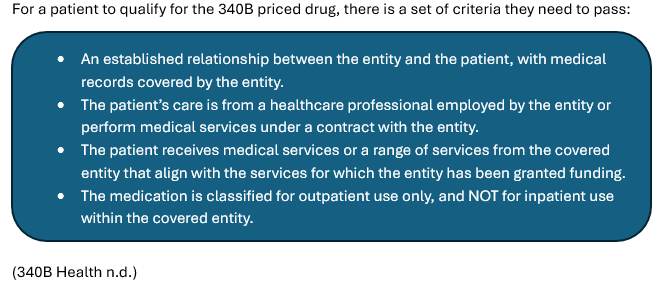
If you’re in the healthcare field, you’ve probably heard of the 340B Drug Pricing Program. Established in 1992 under Section 340B of the Public Health Services Act, this federal program aims to make outpatient medications more accessible for low-income and uninsured patients. Essentially, pharmaceutical manufacturers agree to sell certain drugs at discounted prices to qualify for participation in Medicaid and Medicare Part B, with the Secretary of Health and Human Services overseeing the arrangements. (Rogers 2022).
The eligible providers or participants are so called “covered entities”. These entities must demonstrate they serve a high proportion of low-income, Medicaid, or uninsured patients to qualify. The covered entities are listed below:

The 340B pricing discounts are exclusively available to Medicaid patients, and states are barred from claiming Medicaid rebates on drugs already purchased at 340B prices due to the “duplicate discount” rule. To prevent multiple discounts, there must be checks and balances during billing coordination between states and providers.
Unlike Medicaid, Medicare Part B is not included in the 340B discounts. Manufacturers must participate in both Medicaid and Medicare Part B programs to qualify for 340B pricing. Importantly, Medicare Part B does not receive rebates or discounts under 340B.
Regulations governing drug pricing within the 340B program also establish a maximum allowable charge called the “ceiling price.” This is the highest price a manufacturer can set for outpatient drugs sold to covered entities. The ceiling price is determined using a specific calculation formula.
340B Ceiling Price = Average Manufacturer Price (AMP) – Unit Rebate Amount (URA) (U.S. Department of Health and Human Services n.d.)
The formula has been simplified because it involves several components within the AMP and URA that needed consideration, which I did not include.
The Average Manufacturer Price (AMP) reflects the price reported to CMS from the prior quarter. Meanwhile, the URA is determined by rebates that manufacturers pay to state Medicaid programs. For most brand-name drugs, the URA is at least 23.1% of the AMP, whereas for generic drugs, it’s 13% (Dolan, 2019).
Regarding the use of 340B revenue, there are no strict requirements specified. However, federal grantees operating as covered entities are generally expected to use these funds in accordance with their grant agreement.
This brief report provides an overview of the 340B Drug Pricing Program. For a more comprehensive understanding, please explore additional resources on the subject.
By Nuhro D. Aydin, MBA
January 11, 2026
Works Cited
340B Health. n.d. 340B Health. Accessed December 19, 2025. https://www.340bhealth.org/members/340b-program/overview/.
Dolan, Rachel. 2019. Kaiser Family Foundation. November 12. Accessed December 22, 2025. https://www.kff.org/medicaid/understanding-the-medicaid-prescription-drug-rebate-program/.
Rogers, Hannah-Alise. 2022. “Overview of the 340B Drug Discount Program.” Congress.gov. October 14. Accessed December 20, 2025. https://www.congress.gov/crs-product/IF12232.
U.S. Department of Health and Human Services. n.d. Office of Pharmacy Affairs 340B OPAIS. Accessed December 22, 2025. https://340bpricingsubmissions.hrsa.gov/Help/Manufacturer/Pricing%20Formulas/Pricing%20Formulas.htm.



Leave a comment